
Why You're Not Losing Weight on Ozempic (And What to Do)

You started Ozempic with realistic expectations. Maybe ten pounds in the first month, steady losses after that, and finally a tool that does some of the heavy lifting your last six attempts didn't. Three or four months in, the scale has stopped moving, or worse, it's drifting back up. The dose is the same. The appetite suppression is still there. You're doing everything you were told to do. But the medication that worked so well in month one? Well, that seems to have quietly quit on you.
Here's what we tell every GLP-1 client at GFIT before we change a single thing about their plan: when Ozempic, Wegovy, or Mounjaro "stops working," it is almost never the medication. Nine times out of ten, the culprit is one of five things. And four of them have a fix you can start this week, without a dose change and without giving up.
Stuck on a GLP-1 plateau?
Book a free 15-minute coaching consult with our Winnipeg-based GLP-1 team. We'll review your stall, suggest what to try in the next 14 days, and confirm your insurance coverage on the call.

The 5 Real Reasons Ozempic Stops Working

Reason 1: You stopped eating enough
The first thing GLP-1 medications do is kill your appetite. The second thing they do (and the thing almost nobody warns you about) is take you below the calorie floor your body needs to keep losing fat, which slows down your metabolism.
In the first 4 to 8 weeks on Ozempic, it's normal to eat 30 to 40% less without trying. That works for a while. But around month three, your body adapts. Cortisol creeps up. Thyroid output dips. NEAT, the non-exercise activity that accounts for fidgeting, walking, gesturing, quietly drops. The deficit you used to be running stops being a deficit. And because you still don't feel hungry, you don't notice that you're eating barely above your new lower baseline.
The fix is counterintuitive: you actually need to eat more. Specifically, eat more protein and more total food on three days of the week, then keep the other four at your normal intake. This is the diet break your metabolism needs to reset.
If you have been doing this alone for months and the math keeps moving, this is the moment most clients bring in a Winnipeg nutrition coach to lock the plan.
"I see clients in their fourth month of Ozempic eating 900 calories a day, exhausted, no longer losing weight, and convinced the medication has stopped working. The medication is fine. The problem is that they've backed themselves into a metabolic corner."
Sarah Knight, GFIT GLP-1 & Major Weight Loss Coach
Reason 2: You've lost muscle, not just fat
When the scale moves, we tend to assume it's fat. But on a GLP-1, a meaningful percentage of what you've lost is often actually muscle: sometimes 25 to 40% of total weight lost, depending on your age, your protein intake, and whether you're doing any resistance training.
Muscle is metabolically active tissue. Lose enough of it and your resting metabolic rate drops, your insulin sensitivity worsens, and you become "skinny fat": a smaller version of the body you started with, not a healthier one. The scale still says you've made progress, but your tape measure and your bloodwork tell a different story.
The fix is two-pronged. First, hit 1.6 to 2.2 grams of protein per kilogram of bodyweight per day, even if you don't feel hungry for it. For a 70-kilogram adult, that's 112 to 154 grams of protein daily (see the full protein breakdown for fat loss for how to hit it without forcing the calories). Second, lift weights two to three times a week. Strength training on a GLP-1 isn't optional. It is the difference between losing weight and losing function.
Both inputs are non-negotiable, and they are the backbone of GFIT's GLP-1 coaching program.
Reason 3: You've hit metabolic adaptation
Even people who eat enough and lift weights hit a wall on GLP-1s around month 4 to 6. This is metabolic adaptation, and it's not failure: it’s biology. Your body has noticed it's been in a deficit for months and is dialling down energy expenditure to protect you from what it interprets as a famine.
The signs cluster:
- Weekly weight loss slows from 1 to 2 pounds to 0 to 0.5 pounds.
- You're colder than usual, especially your hands and feet.
- Your energy is lower; you feel "tired but wired."
- Sleep quality declines; you struggle to fall asleep or experience 3 am wakeups.
- Strength suffers, and your workouts feel harder and harder.
The fix is a structured 7 to 14-day diet break, eating at maintenance calories, not in a deficit, and then resuming your normal plan. Counterintuitively, this restarts weight loss faster than continuing to push the deficit. Our GLP-1 coaches can run the math on your maintenance number; if you're doing it alone, multiply your body weight in pounds by 13 to 15 for a rough estimate.
Reason 4: Your dose has plateaued
This is the only reason on the list that is actually about the medication. GLP-1 medications work on a dose-response curve. The 0.5 mg starter dose of Ozempic produces about 60% of the appetite suppression of the 2.0 mg dose. If you've been stuck at 1.0 mg for six months because the side effects were rough at the start, you may be undermedicating.
This is a conversation with your prescriber, not your coach. Bring three things to the appointment:
- Your weight trend over the last 90 days (a phone screenshot is fine).
- Your current side-effect tolerance: nausea, fatigue, GI changes.
- Your goals over the next 90 days.
A dose increase isn't always the answer. Sometimes the right move is a longer stay at the current dose; sometimes it's switching from Ozempic to Wegovy or Mounjaro. But it should be on the table, and your coach should be in the loop, because a dose change usually requires a change in nutrition, too.
Reason 5: The behaviour piece never changed
The hardest reason to hear, and the most common: Ozempic worked because it muffled your appetite. But you never actually changed how, why, or what you eat. So when the medication's effect plateaus (and it eventually does for everyone), you're left with the same eating patterns that put you here in the first place. Only now with a smaller stomach.
If you go off Ozempic without having built new habits, you will regain. The data on this is brutally consistent: roughly 65% of weight lost on a GLP-1 is regained within 12 months of stopping the medication.
The fix is the slowest and the most important. While the medication is doing the heavy lifting, use that window to rebuild your relationship with food: meal structure, hunger awareness, emotional eating triggers, protein-first plates, and alcohol patterns. The medication buys you the runway. What you do with that runway determines whether the fat loss lasts.
One of our Winnipeg members, Jill, lost 38 pounds on Ozempic in her first six months. By month nine, she had stopped losing and panicked. We didn't change her medication. We changed three things: her breakfast went from a coffee to 30 grams of protein, she started lifting twice a week, and she got eight hours of sleep instead of six. The scale started moving again within three weeks.
If you’re starting to think about your exit strategy, here is how to come off Ozempic safely.
The 14-Day Reset That Restarts Progress
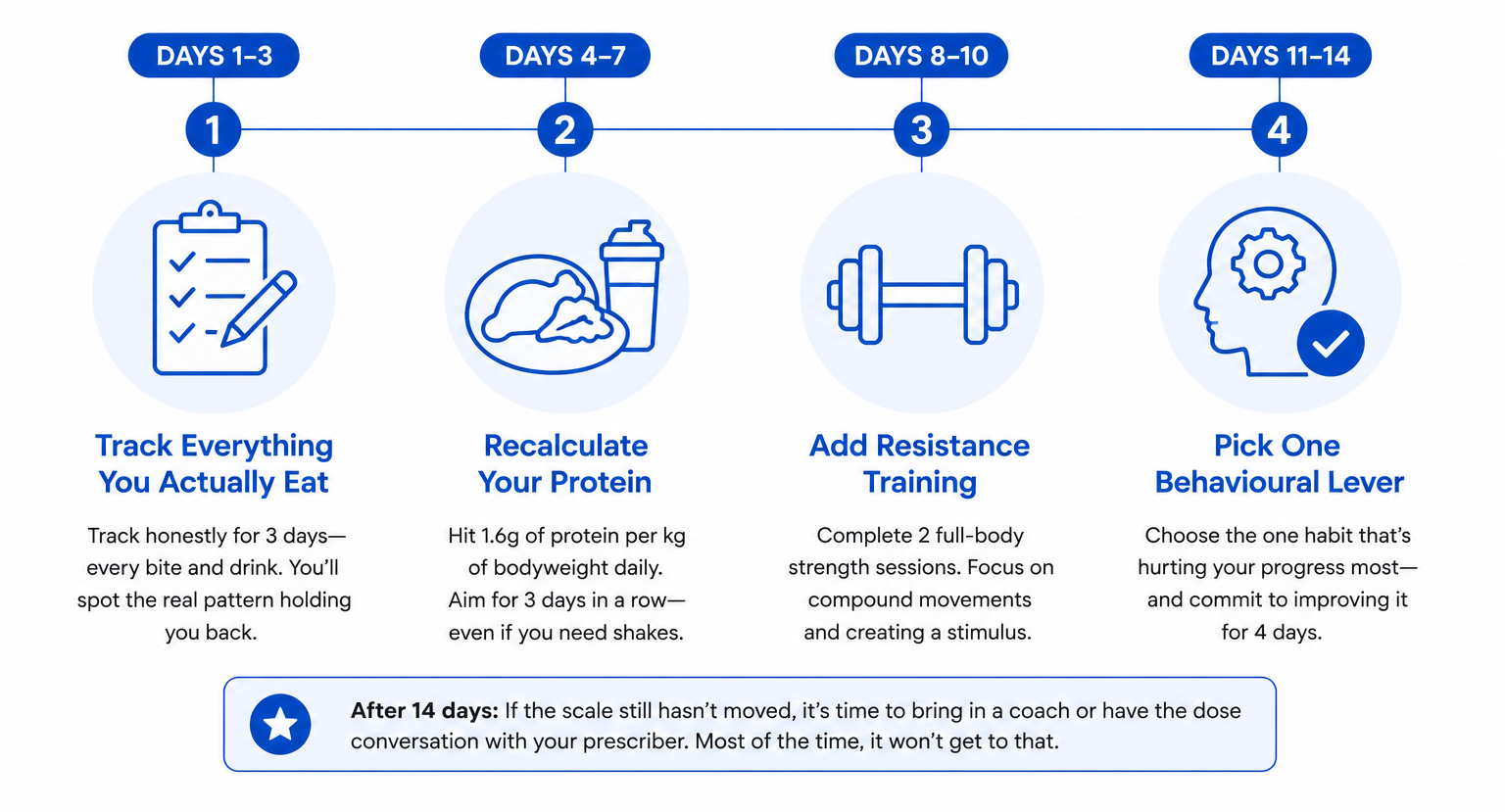
Before you call your prescriber, run this 14-day audit: we call this the GFIT 14-Day Reset. The four steps? Track your food for three days, recalculate protein, add resistance training, and pick one behavioural lever. We use a version of this with every GFIT GLP-1 client who hits a plateau.
Days 1 to 3: Track everything you actually eat
Not what you're supposed to eat. What you're actually eating. Honest tracking, every bite. Most plateaued clients discover they're either eating much less than they thought (Reason 1) or much more (sneaky calories from coffee additions, snack-while-cooking, restaurant portions you eyeballed). You only need three days to spot the pattern.
Days 4 to 7: Recalculate your protein
Multiply your bodyweight in kilograms by 1.6. That's your minimum daily protein in grams. Hit it three days in a row, even if it means a protein shake or two. If you can't get there from food, that's information. It usually means you need a coach-built meal structure rather than another willpower attempt.
Days 8 to 10: Add resistance training
Two full-body sessions. Focus on compound movements like squats, hinges, pushes, and pulls, plus a few minutes of core work. If you've never trained before, this is the moment to either join a gym with a coach or follow a structured beginner program. The goal isn't intensity. It's creating a stimulus.
Days 11 to 14: Pick one behavioural lever
Sleep, alcohol, stress eating, restaurant frequency: identify the one that's most clearly compromising your plan and fix it. One. Not all four. The most common culprit we see in this stage is alcohol creeping back in once nausea improves around month three.
If at the end of 14 days the scale still hasn't moved, that's when you bring in a coach or have the dose conversation with your prescriber. Most of the time, it won't get to that.
When to Bring in Professional Help
DIY works, until it doesn't. Three signs you should bring in a Winnipeg-based coach with GLP-1 experience:
- You've been stuck for 90+ days despite the 14-day reset.
- You're afraid to come off the medication and don't have a plan for what happens after.
- You're losing weight, but your strength, energy, or bloodwork is worse than when you started.
At GFIT, our GLP-1 coaching program is built specifically for this: clients on Ozempic, Wegovy, or Mounjaro who want to make sure the weight stays off and the body that's left is stronger, not just smaller. Most of our GLP-1 clients are insurance-covered, which means a typical 12-week program runs little to nothing out of pocket if you have benefits through Manitoba Blue Cross, Canada Life, Sun Life, Manulife, or Green Shield.
Get a second opinion on your GLP-1 stall
Book a free 15-minute consult with our Winnipeg-based GLP-1 team. We'll look at what's stalling progress, suggest your next 14 days, and confirm your insurance coverage on the call. No pressure, no upsell.
Frequently Asked Questions
A protein shake counts. Most clients who report "I can't eat breakfast" can drink 30 to 40 grams of protein in a smoothie or in coffee. If even liquid is uncomfortable first thing, push your first protein touchpoint to 10 or 11 am, but don't skip the day's first protein hit entirely.
Most likely yes. The evidence for creatine monohydrate during weight loss is strong, the safety profile is excellent, and 5 grams per day is well-tolerated by most GLP-1 patients. Confirm with your prescriber if you have kidney concerns or are on other medications.
Definitely. Protein alone isn't enough. Without resistance training (two to three sessions a week), you will still lose meaningful muscle even with adequate protein intake. Both inputs are required, and the training is the non-negotiable one most people underestimate.
Whey or casein protein powder mixed into a shake is the single most reliable option for most clients. High protein, low volume, no chewing, easy to flavour blandly if strong tastes are off-putting. Greek yogurt and cottage cheese are close seconds.
Between 1.6 and 2.2 grams of protein per kilogram of body weight per day. For a 75-kilogram (165-pound) adult, that works out to 120 to 165 grams daily. Go to the lower end if you're under 50 and active, the higher end if you're over 50 or in a steeper calorie deficit.
The signs cluster: weight loss slows, you feel cold, your energy drops (separate from medication side effects), sleep quality worsens, and workouts feel harder. If three or more of those have appeared in the last six weeks, adaptation is the most likely explanation, not a medication failure.
Technically yes, but do so at your own risk. You'll lose more muscle than fat, your metabolism will drop, and you'll regain weight aggressively if you stop the medication. Resistance training determines whether the weight you lose is mostly body fat or mostly muscle. Two resistance training sessions a week is the minimum we recommend for any GLP-1 client.
Maybe, but only after ruling out the five non-medication reasons in this article. Talk to your prescriber with 90 days of weight data, your current side-effect tolerance, and your goals for the next 90 days. A coach can help you assemble that picture before the appointment.
In clinical trials, average weight loss on semaglutide over 68 weeks at full dose (2.4 mg, the Wegovy dose) was about 14.9% of starting bodyweight. Weekly losses of 0.5 to 1 pound after the first month are normal and sustainable. Losses much faster than that often mean muscle is going with the fat.
In roughly 90% of cases, the medication is still working, but one of five things has changed underneath it: you're eating below your metabolic floor, you've lost muscle alongside fat, you've hit metabolic adaptation, your dose needs adjusting, or the behavioural side never shifted. The fix usually doesn't require a dose change.




Book a call with our Wellness Coordinator to learn more



