
How to Eat on a GLP-1 Without Losing Muscle

How to Eat on a GLP-1 Without Losing Muscle
GLP-1 medications make restricting calories easier. That's the whole point, they help turn down the overwhelming food noise and curb your appetite.
But somewhere around week six on Ozempic, Wegovy, or Mounjaro, most people notice the same thing: nothing tastes good, nothing feels appealing, and the protein targets your coach or your search results keep mentioning feel laughably out of reach when half a chicken breast is the most you can stomach. The risk underneath that gap is real: muscle loss. And the cost of getting it wrong is far steeper than most people realize.
Here's the short version: to protect muscle on a GLP-1, you need 1.6 to 2.2 grams of protein per kilogram of bodyweight per day, spread across three to four meals (or shakes). And you almost certainly need structured meals to get there. The rest of this article is the exact playbook our GFIT GLP-1 coaches use with our clients to help them hit their protein goal when their appetite is muted: what to eat, when to eat it, and our top tips on how to make it doable when food just isn't appealing.
Want this dialled in for you personally?
Book a free 15-minute consult with our Winnipeg-based GLP-1 nutrition team. We'll review your current protein intake, suggest a 4-step meal structure that fits your day, and confirm your insurance coverage on the call.

Why Muscle Loss Happens on GLP-1s (And Why It Matters More Than You Think)
Every time you lose weight, some of what you lose is muscle, and to be clear, that's actually true on any diet, with or without medication. What makes GLP-1s different is the speed of the muscle loss: you can lose weight quickly enough that your body doesn't have time to preferentially burn fat. Plus, the intense appetite restriction means that you can eat so little that your protein intake collapses, and both of those factors push the muscle-loss percentage far above what typical diets do.
In clinical studies of semaglutide and tirzepatide, lean mass loss has accounted for roughly 25 to 40 percent of total weight lost. For a person losing 50 pounds, that's potentially 12 to 20 pounds of muscle gone. And most of it never comes back without deliberate work after the fact.
When you’re desperate to see the scale move, it’s easy to see any weight loss as a good thing. But here are four reasons why muscle loss matters more than people think:
- Muscle is your largest metabolic organ. Less of it means a lower resting metabolic rate, which makes future weight maintenance much harder: the lower your metabolism goes, the less you can eat without gaining weight. This makes maintaining your new lower weight much harder, and weight regain much more likely.
- Muscle drives insulin sensitivity. Losing muscle worsens the exact metabolic risk most GLP-1 patients are trying to treat in the first place.
- Muscle = strength and functionality. Mobility, balance, and independence come from maintaining strength and muscle.
- From an aesthetic perspective, weight loss that is mostly muscle tends to result in the opposite of the lean, toned physique most people are after: it leads to the dreaded ‘skinny fat’ body that’s just essentially a smaller (but still fat) version of the way you started.
www.gfitwellness.ca/glp-1-coaching-winnipeg
The Protein Math
Forget the generic "eat more protein" advice. Here's the number that actually matters: 1.6 to 2.2 grams of protein per kilogram of bodyweight per day. You can stick to the lower end of that range if you're under 50 and lifting weights twice a week; you’ll need the higher end if you're over 50, in a steeper deficit, or new to strength training.
Let’s say you’re a 75-kilogram (165-pound) adult:
- Low end: 75 × 1.6 = 120 grams of protein per day.
- Mid range: 75 × 1.9 = 143 grams per day.
- High end: 75 × 2.2 = 165 grams per day.
Most of our GLP-1 clients land between 130 and 160 grams of protein per day. The number itself might sound doable, but as GLP-1 users know, distributing it across the day when you have no appetite can be a real challenge. That's the actual problem we need to solve.
"The single biggest factor that predicts whether a GLP-1 client keeps their muscle isn't which medication they're on. It's whether they have a meal structure they can actually follow. When food doesn't appeal to you, we have to get creative to find ways to get protein in, that’s where our 4-point plan comes in.". Riel Hildawa GFIT GLP-1 nutrition coach
The GFIT 4-Point Structure for GLP-1s
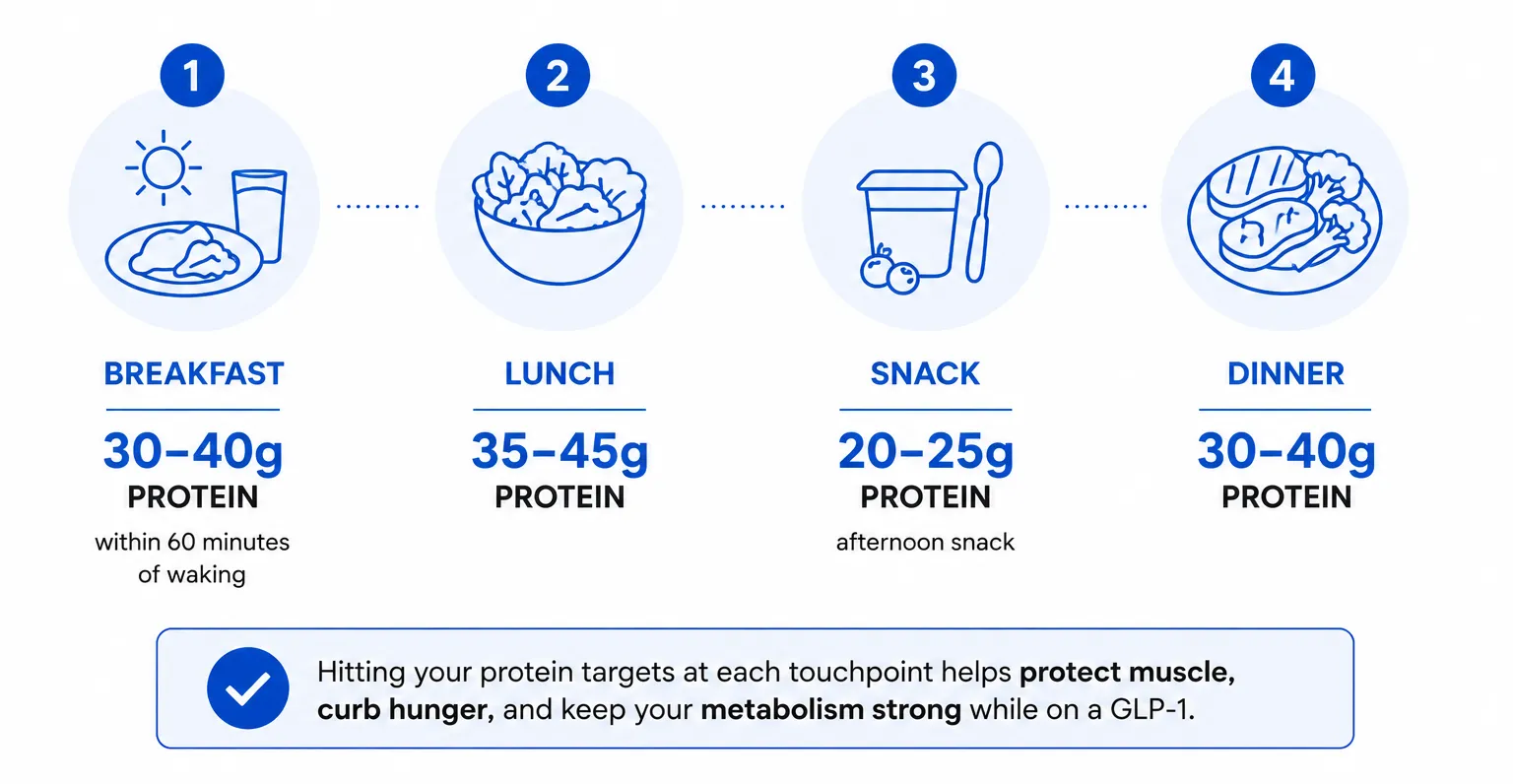
When appetite is suppressed, willpower will not get you to 140 grams of protein a day: we need to create a consistent, repeatable structure. Every GLP-1 client at GFIT operates on what we call the GFIT 4-Point Meal Structure, regardless of preference or schedule.
Touchpoint 1: A protein-forward "breakfast" within 60 minutes of waking
This is the hardest meal on a GLP-1, because the appetite suppression effects mean most people don’t wake up hungry. The goal here is to get in 30 to 40 grams of protein, achieved with the smallest physical volume of food possible. Three options that work reliably:
- 2 eggs + 1 single-serve container of Greek yogurt + 1 scoop of protein powder stirred into coffee (~38 g protein).
- 1 scoop whey isolate in ultrafiltered milk + 2 hard-boiled eggs (~45 g).
- Cottage cheese (3/4 cup) + 1 scoop collagen + a small handful of berries (~35 g).
If you genuinely cannot eat solid food in the morning, a high-protein drink can be subbed in. But note that a skipped breakfast almost guarantees that you’ll miss your daily protein target. That's the most consistent pattern we see in client food logs.
Touchpoint 2: Lunch, protein-anchored, eaten while you have some appetite
The biggest mistake you can make at lunch on a GLP-1 is grazing. Pick one protein anchor, build the rest of the plate around it, and eat the protein first. Target: 35 to 45 grams.
- 150 g grilled chicken breast + half a sweet potato + steamed broccoli (~40 g).
- 1 can tuna in water + 1 cup edamame + half an avocado on a bed of greens (~38 g).
- 4 oz extra-lean ground turkey + 3/4 cup quinoa + roasted vegetables (~36 g).
The eat-protein-first rule matters because once you feel full on a GLP-1, force feeding yourself feels impossible. Think protein first, vegetables second, carbs last.
Touchpoint 3: A planned afternoon protein snack
This is the touchpoint most people skip. Don't! A 20- to 25-gram protein snack somewhere in the 3 to 5 pm window is the single most predictive habit separating clients who hit their daily protein from clients who don't. Options that travel and don't require chewing through a full meal:
- 1 protein bar (look for 20+ g protein and under 10 g sugar. Quest, Built Bar, Pure Protein).
- 1 scoop whey isolate shaken in a bottle of water or ultrafiltered milk.
- 1 cup Greek yogurt + 1 tablespoon nut butter.
- 100 g cottage cheese with a drizzle of honey or hot sauce.
Touchpoint 4: Dinner, smaller than you used to eat, still protein-anchored
By dinner, most GLP-1 patients are at peak fullness. Aim for 30 to 40 grams of protein and accept that your carb and vegetable volume will likely be smaller than it used to be. That's fine. The total daily protein number matters more than your dinner plate looking "normal." If your old plate was 1/3 protein, 1/3 starch, 1/3 vegetables, on a GLP-1 it becomes 1/2 protein, 1/4 starch, 1/4 vegetables. Remember - your “normal” plate is what got you into trouble in the first place.
www.gfitwellness.ca/online-nutrition-coaching-winnipeg
Foods That Work When Nothing Tastes Good
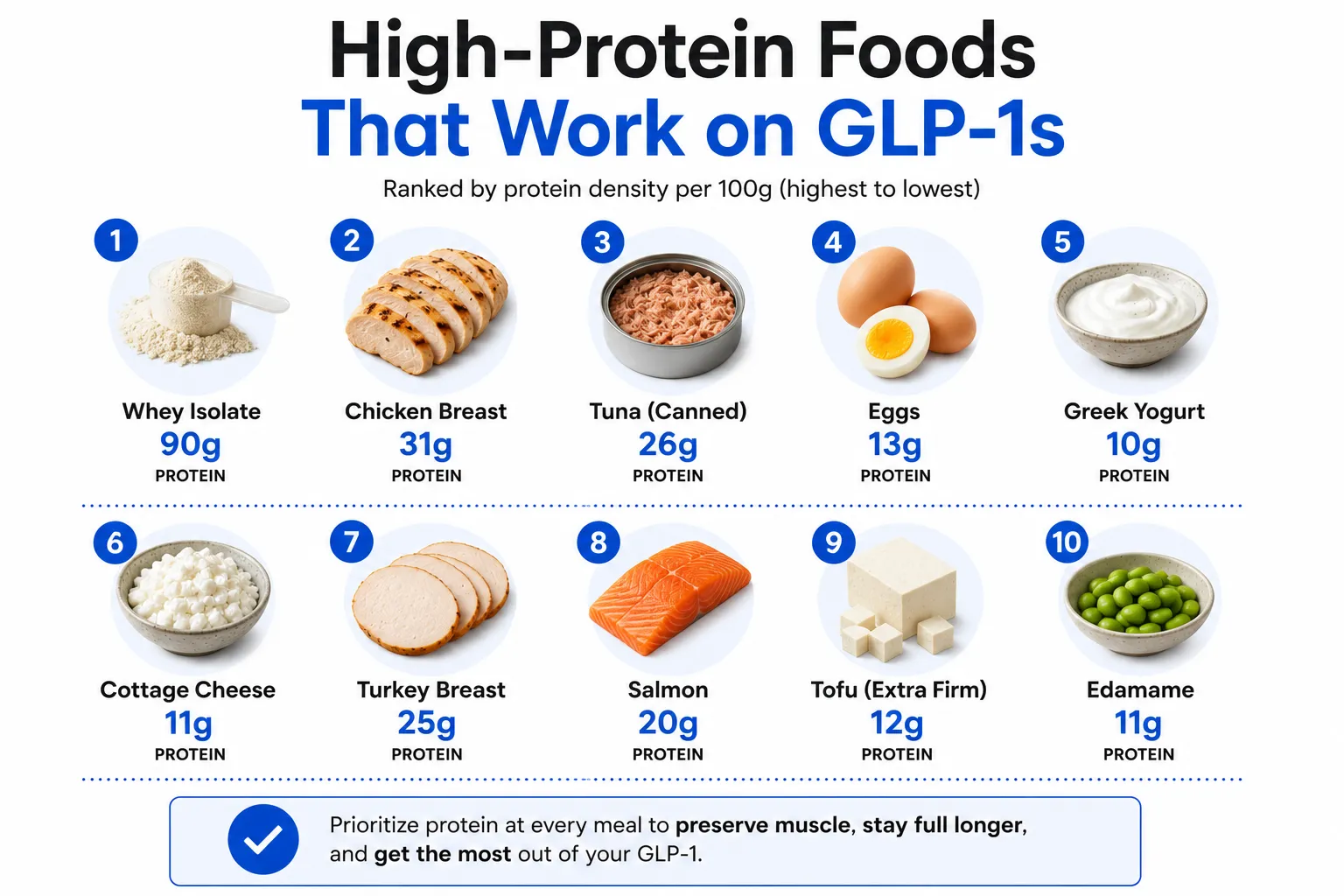
GLP-1 patients describe their food experience differently than non-users do. We commonly hear from clients that meat tastes metallic, fatty foods feel heavy in a new way, sweet foods taste cloying, and anything overly aromatic triggers nausea. The foods most likely to stay palatable through GLP-1 treatment share these three properties: high protein density, mild flavour, and neutral temperature options.
The reliable performers we recommend to most of our clients:
- Greek yogurt. Liberte 0%, Oikos Triple Zero, PC plain. Available at every Winnipeg grocery store.
- Cottage cheese. Western Family, Sealtest, or Western Creamery are widely available.
- Whey isolate powder. Chocolate or vanilla; cleaner brands like Isopure, Dymatize Iso100, or NutraBio.
- Egg whites and whole eggs. Any form.
- Chicken breast. Slow-poached or sous vide. Texture matters when appetite is low; dry, grilled chicken often stops working around month two.
- Canned tuna or salmon in water.
- Lean ground turkey or chicken.
- White fish. Cod, tilapia, haddock. Mild flavour and fast to cook.
- Edamame. Frozen, microwave-steamed in 4 minutes.
- Tofu. Firm, pressed and pan-seared.
- Protein bars. Quest, Built Bar, RX Bar, Pure Protein.
What tends to stop working around month two or three on most clients: red meat (due to the texture and density), eggs, oily fish like salmon, and fatty pork. Know that this isn’t typically a permanent change: palatability often returns at lower medication doses or after stopping. But during active use, lean and mild proteins tend to work better.
The Other Critical Piece Of The Puzzle: Strength Training
It’s critical to understand that protein alone won't preserve muscle on a GLP-1.You need to send your body a consistent signal to build and preserve muscle, or your body will let go of it. The minimum effective dose is two full-body resistance training sessions a week, 30 to 40 minutes each, focused on compound movements: a squat or leg press, a hinge or deadlift, a push, a pull, and a few minutes of core work.
You don't need a personal trainer or a fancy gym to do this, But you do need a structured program built on progressive overload.Our coaches can design one that utilizes bodyweight, bands, dumbbells, machines, or whatever you have access to.
If you've never strength trained before, that’s okay, but it's time to learn. A GFIT coach can make you a custom program, covered by insurance benefits to boot.
The 5 Most Common Eating Mistakes on a GLP-1
- Skipping breakfast; this almost always leads to missed daily protein, even in clients who eat the rest of their meals.
- Liquid calories( that aren't protein). Coffee with cream, kombucha, juice - these take up gut space without meaningfully contributing to your protein target, and should be skipped
- Eating vegetables first. This fills you up before you've hit your protein anchor - and once full on a GLP-1, it’s incredibly hard to keep going.
- Empty calories. A sleeve of crackers is technically eating, but it doesn't move you toward your goal.
- Skipping the afternoon protein snack; this is the single most predictive habit separating clients who hit protein targets from those who don't.
Learn from one of our Winnipeg clients: let’s call him James. James was six months into Wegovy, had lost 42 pounds, and was thrilled with his scale progress. But his DEXA scan told a different story: he'd lost 11 pounds of lean mass. James really struggled with his appetite due to the high dose of medication he was on, so we knew we had to make small, doable changes. We added one breakfast shake, one afternoon protein bar, and two 30-minute lifting sessions a week (critical to preserve muscle). Three months later, his next DEXA showed he'd regained 4 pounds of muscle and was still losing body fat.
When to Bring in a Coach
You don't need a coach to tell you to eat more chicken, but you may need one if any of the following are true:
- You've been on a GLP-1 for 60+ days and have no idea whether you're hitting your protein goal.
- The food list above eliminates most of what you actually like to eat.
- You're losing weight but feeling weaker, more tired, or sleeping worse than when you started.
- You're approaching your goal weight and are nervous about what happens to your eating and habits when the medication taper begins.
At GFIT, our GLP-1 nutrition coaching is built around the GFIT 4-Point Meal Structure above, customized to your appetite at your current dose, your food preferences, and your daily schedule. Most of our Winnipeg clients are insurance-covered through Manitoba Blue Cross, Canada Life, Sun Life, Manulife, or Green Shield, which means the coaching itself usually runs little to nothing out of pocket.
Get your eating plan built around your GLP-1
Book a free 15-minute consult with our Winnipeg-based GLP-1 nutrition team. We'll build a 4-touch structure that fits your actual day, recommend foods that work at your current dose, and confirm your insurance coverage on the call.
Frequently Asked Questions
Between 1.6 and 2.2 grams of protein per kilogram of body weight per day. For a 75-kilogram (165-pound) adult, that works out to 120 to 165 grams daily. Go to the lower end if you're under 50 and active, the higher end if you're over 50 or in a steeper calorie deficit.
Whey or casein protein powder mixed into a shake is the single most reliable option for most clients. High protein, low volume, no chewing, easy to flavour blandly if strong tastes are off-putting. Greek yogurt and cottage cheese are close seconds.
Definitely. Protein alone isn't enough. Without resistance training (two to three sessions a week), you will still lose meaningful muscle even with adequate protein intake. Both inputs are required, and the training is the non-negotiable one most people underestimate.
Most likely yes. The evidence for creatine monohydrate during weight loss is strong, the safety profile is excellent, and 5 grams per day is well-tolerated by most GLP-1 patients. Confirm with your prescriber if you have kidney concerns or are on other medications.
A protein shake counts. Most clients who report "I can't eat breakfast" can drink 30 to 40 grams of protein in a smoothie or in coffee. If even liquid is uncomfortable first thing, push your first protein touchpoint to 10 or 11 am, but don't skip the day's first protein hit entirely.


.webp)

Book a call with our Wellness Coordinator to learn more



