
Coming Off Ozempic: How to Actually Keep the Weight Off

Coming Off Ozempic: How to Actually Keep the Weight Off
Everyone who starts a GLP-1 eventually thinks about stopping. Maybe your insurance coverage changed. The cost of the medication rose. The side effects started to compound. Maybe a prescriber decides the medication has done its job, or maybe you hit your goal, and you’re ready to see what life is like on the other side. Whatever the trigger, the question that follows is the same one. And it's the one that keeps people awake at night: will I just gain it all back?
Here's the short version. Coming off Ozempic, Wegovy, or Mounjaro is a 90- to 180-day project, not one brief moment. The patients who keep the weight off don't have better willpower than the ones who don't. They have a structured taper plan that addresses four predictable phases (medication, appetite, behaviour, and identity). They keep training and tracking through all four, and they almost always have a coach in their corner during the high-risk window of weeks 5 to 12. The article that follows is that plan.
Planning to come off Ozempic in the next 6 months?
Book a free 15-minute consult with our Winnipeg-based GLP-1 maintenance team. We'll walk through your taper timeline, build a Phase 2 plan, and confirm your insurance coverage on the call.

The Uncomfortable Data on Weight Regain
The STEP-1 extension trial is the longest published follow-up of patients stopping semaglutide. Here’s what it found: participants regained roughly two-thirds of the weight they had lost within 12 months of stopping the medication. The signal was clear: cravings returned within weeks, eating volume crept back, exercise habits eroded, and as the appetite-suppression disappeared, weight climbed.
That statistic gets quoted everywhere, usually as a horror story, and sometimes as an argument for staying on the medication forever. But neither framing is quite right. The trial design didn't include a structured maintenance program. Participants got the medication, and then they got nothing. The regain numbers tell us what happens in the absence of intervention; not what's inevitable for everyone.
What the trials don't tell you is what happens when you replace the medication's effect with deliberate structure: protein, training, sleep, accountability, and a tapered-down behavioural plan. In our GFIT GLP-1 coaching cohort, the maintenance numbers look meaningfully different. Most clients hold within 5 to 10 percent of their target weight at the 12-month mark.
The underlying problem is straightforward. The mechanism that drove your weight loss is leaving the building, and the behaviours that have to fill the gap don't exist yet. That's the entire problem our coming-off-Ozempic planning is trying to solve.
The GFIT 4-Phase Taper
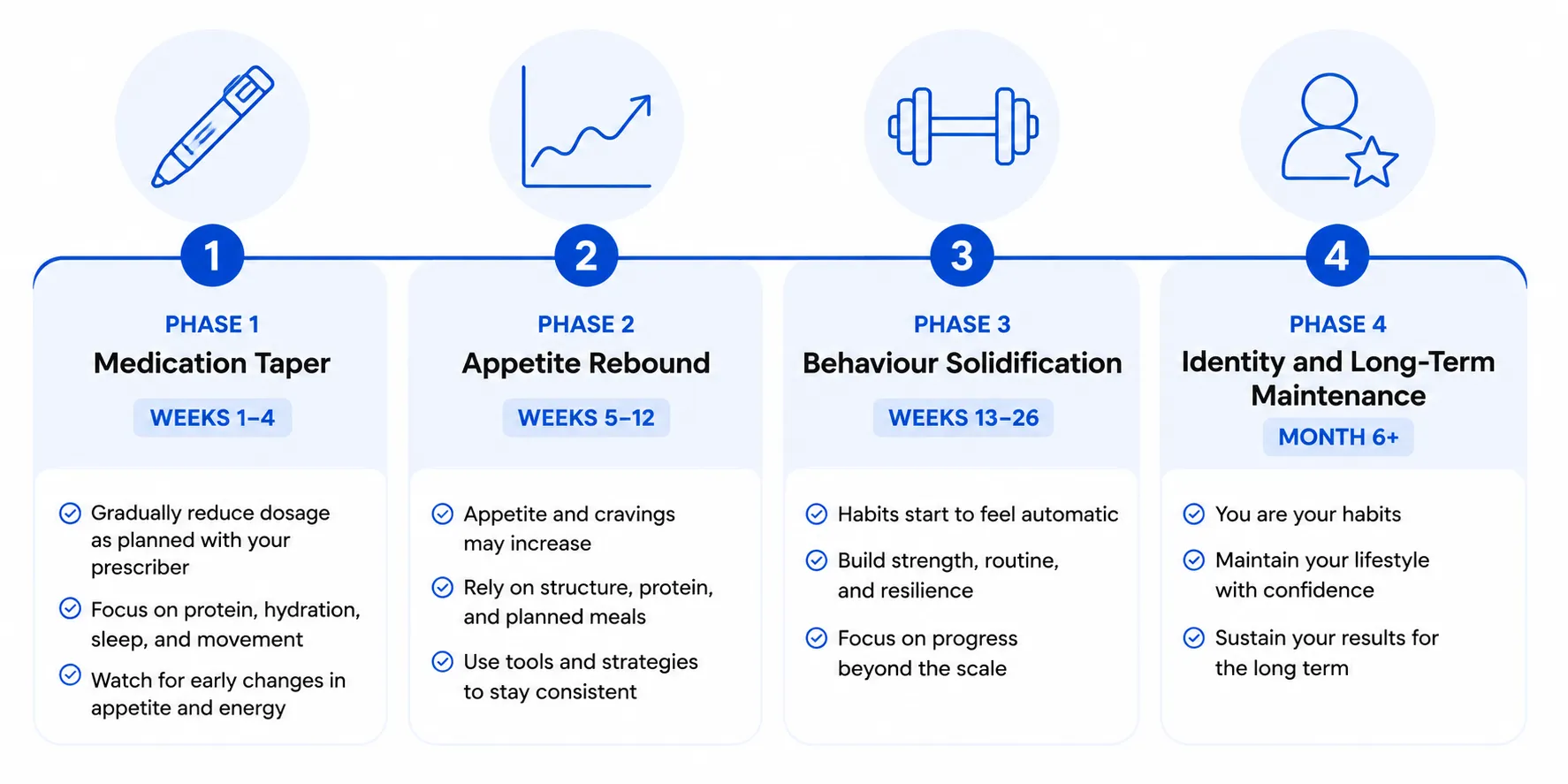
Most people treat coming off Ozempic as a single event, and this is a big mistake. The alternative? The GFIT 4-Phase Taper. Coming off is a transition with four distinct phases, each with its own challenges, and its own non-negotiables.
PHASE 1: The Medication Taper (Weeks 1 to 4)
Semaglutide has a half-life of about a week. After your last dose, the medication remains biologically active in your system for roughly 5 to 7 weeks. The appetite suppression doesn't end on day one: it fades over a month or more.
What to do during Phase 1:
- Coordinate with your prescriber on a step-down rather than a hard stop. For example, 2.0 mg → 1.0 mg → 0.5 mg → off, over six to eight weeks. Tapers consistently produce less severe appetite rebound than abrupt cessation.
- Track your daily food intake honestly during this window. You'll be surprised how little you're eating, which is the problem Phase 2 has to address.
- Lock in your training program now. Phase 2 is too late to start strength training.
- Book a 90-day check-in with your prescriber for the date of your last dose, plus a 6-month check-in. Don't wait for problems to arise to get this appointment on the calendar.
What not to do during Phase 1:
- Don't use your still-suppressed appetite as an excuse to eat less and lose more weight. That backfires hard in Phase 2.
- Don't stop training because you've hit your goal weight. Muscle is your insurance policy against fat regain.
PHASE 2: The Appetite Rebound (Weeks 5 to 12)

This is the danger zone, where we predictably see clients struggle the most. Around week four to six, your appetite returns, and it’s often sudden, dramatic, and paired with strong cravings. Most patients describe this feeling as a drastic shift, with the food noise returning stronger than ever.
It’s important to understand that this is actually a predictable hormonal event, and not a willpower failure. Ghrelin (the hunger hormone) climbs back to baseline and sometimes overshoots, while leptin sensitivity (the satiety hormone) takes longer to recalibrate. Your hunger feels louder than it did pre-medication, and your fullness feels quieter. Both signals are unreliable for the first six to eight weeks after full medication clearance.
The patients who get through Phase 2 well do four things consistently:
- Eat at maintenance calories, not in a deficit. Trying to maintain a deficit through Phase 2 will fail, and the resulting binge will set the tone for the next year.
- Front-load protein: 30 to 40 grams at breakfast is the single most effective hunger-management lever we have access to.
- Walk daily: 8,000 to 12,000 steps is the goal. Walking blunts your appetite, burns calories, and doesn't drive the rebound hunger that more aggressive cardio can.
- Sleep 7 to 9 hours. Sleep deprivation amplifies ghrelin, and this is the worst possible eight-week window for that.
This is where a coach earns their entire fee. This hunger rebound is the most predictable failure point in the entire GLP-1 journey, and it's almost completely manageable with the right structure in place before it hits. The patients who hit Phase 2 with no plan are the ones who quietly regain over the following nine months.
"Setting realistic expectations for Phase 2 is the conversation I have most often with clients. They come in around week five, panicked because the cravings are back, and they're afraid they've lost everything. But they haven't. They've hit a predictable hormonal event, and we have a proven protocol to get them through it. Most clients are stable again by week ten." Amanda Chartrand, GFIT Coach - Major Weight Loss, GLP-1 Support & Healing Your Relationship with Food
PHASE 3: Behaviour Solidification (Weeks 13 to 26)
By week 13 the medication has fully cleared, your appetite has stabilized into its new normal, and the question now shifts into one about behaviour. Phase 3 is about seeing whether the eating and training habits you’ve built are durable enough to go the distance, now that the training wheels of the medication have been removed.
What to do during Phase 3:
- Move from "maintaining weight" thinking to "consolidating habits" thinking. The goal is making the new behaviours unconscious, not white-knuckling them every day.
- Add a second weekly strength training session if you've only been doing one. Three is the target for long-term body composition maintenance.
- Track weight weekly, not daily. The noise of daily fluctuations distorts judgment and feeds anxiety.
- Identify your top two or three risk situations (holidays, travel, work stress, family meals) and pre-plan exactly how you’re going to handle them.
PHASE 4: Identity and Long-Term Maintenance (Month 6 and beyond)
The patients who keep the weight off long-term think of themselves as people who train consistently, eat protein daily and prioritize their health. The medication was a tool that helped them build the runway to their new identity; not a lifelong crutch.
That identity shift is the long game. It usually takes 9 to 18 months to fully settle in, and it's accelerated by:
- Strength training built on progressive overload and getting stronger
- A coach and/or community that reinforces your new identity. Surround yourself with people who eat the way you eat and train the way you train.
- Periodic body composition tracking (DEXA, calipers, etc.). Body composition is a more accurate measure of progress and success than scale weight.
- Annual bloodwork to track metabolic markers. The medication treated more than the number on the scale; you want to know what’s happening with these markers too.
The Non-Negotiables Through All Four Phases
A few things don't change, regardless of which phase you're in:
Protein
1.6 to 2.2 grams per kilogram of bodyweight per day, distributed across three to four meals. Protein is the most satiating macronutrient and the foundation of muscle preservation. For a 75-kilogram adult, that's 120 to 165 grams per day.
Strength training
Two sessions per week minimum (ideally three). This is the difference between maintaining or progressing your body composition, or slowly losing muscle while gaining fat. And both can happen silently while nothing changes with your scale weight.
Sleep
The single most underrated lever in weight maintenance: aim for 7 to 9 hours. Sleep deprivation raises ghrelin, lowers leptin, increases cortisol, and tanks workout performance.
Tracking minimum-viable metrics
Think weekly weight, monthly waist measurement and quarterly bloodwork. Most regain happens silently. 200 extra calories per day for 90 days adds up to roughly five pounds of fat. It might not be visible day-to-day, but it’s painfully clear at the three-month check-in.
Honesty with food intake
This is the lever most people quietly stop using once the medication is gone. The discipline of honest tracking through the first six months post-medication is the difference between catching drift early and discovering it after it's compounded and it’s too late.
When You Probably Shouldn't Come Off Yet
The default cultural assumption is that GLP-1s are a temporary tool - and while that's true for some patients, it’s wrong for others. Coming off makes the most sense when:
- You've reached your goal weight or a clinically reasonable target.
- Your metabolic markers (i.e. A1C, lipids, blood pressure, liver enzymes) have meaningfully improved.
- You have a maintenance plan ready to deploy.
- You have at least three months of consistent training and eating habits already in place.
Coming off may not make sense when:
- You're stopping because of cost or insurance pressure, but haven't met your goal.
- You don't have a maintenance plan.
- You've never built a training habit during the medication phase.
- Your underlying metabolic condition (Type 2 diabetes, severe obesity, fatty liver disease) is still active, and the medication is treating it.
This is a prescriber conversation, not a coach conversation, but it's a conversation worth having before you make the call. And a coach can help you assemble the picture before the appointment with your provider.
Where Coaching Actually Earns Its Fee
The cost of GFIT GLP-1 maintenance coaching is, for most Winnipeg clients, zero out of pocket if they have benefits through Manitoba Blue Cross, Canada Life, Sun Life, Manulife, or Green Shield. Even at full price, it's a fraction of what continuing the medication would cost over a year.
What coaching delivers during the taper that DIY can't:
- A structured Phase 2 appetite-rebound plan, customized to your food preferences, schedule, and history.
- Weekly accountability through the highest-risk 12 weeks, when most patients lose contact with their plan.
- A pre-built protein meal structure you can default to when willpower drops.
- Reverse-dieting math: help making that crucial transition where you gradually increase calories from your deficit back to maintenance calories without triggering rebound fat gain.
- Coordination with your prescriber when dose adjustments or restarts come up.
- A real plan for the first holiday season, the first big work trip, the first family vacation post-medication.
One of our Winnipeg clients hit her goal weight and finished her Wegovy program in September. She came to us in October with a coaching plan built around the upcoming holidays, her January travel schedule, and her tendency to skip breakfast when life got busy. Nine months later, at her July check-in, her weight was 2 pounds under her target, and her muscle mass was up. The plan did its job, and she was thrilled with the results.
Build your customized taper plan, with a coach who has done this hundreds of times
Book a free 15-minute consult with our Winnipeg-based GLP-1 maintenance team. We'll map your 4-phase taper, identify your Phase 2 risk window, and confirm your insurance coverage on the call.
Frequently Asked Questions
Most clinical protocols suggest at least 12 months of maintained weight loss before considering a taper. Coming off earlier is associated with faster fat regain. That said, the right time to come off is a prescriber decision based on your goals, your metabolic markers, and the readiness of your maintenance plan, not a generic timeline.
Without a structured maintenance plan, the published data suggests roughly two-thirds of lost weight is regained within 12 months. With a structured taper that includes coaching, strength training, and tracked eating, regain rates are dramatically lower. Most of our GFIT clients hold within 5 to 10 percent of their target weight at the 12-month mark.
Taper. For example, reducing from 2.0 mg to 1.0 mg to 0.5 mg over six to eight weeks. This approach reduces the severity of the appetite rebound and gives you time to build habits while the medication is still partially active; hard stops are consistently associated with worse regain.
Weeks five to eight are the most-cited danger window in our coaching practice. The medication has fully cleared from your system, appetite has returned (often dramatically), and the cravings for previously-suppressed foods can be intense. This is exactly when most regain begins, and exactly when having a structured plan matters most.
Yes. Many patients cycle on and off based on weight trajectory, life circumstances, and prescriber guidance. Restarting is generally well-tolerated. If you find yourself needing to restart more than once, that's a signal the underlying maintenance plan needs more work, not that you've failed.




Book a call with our Wellness Coordinator to learn more



