
Why Weight Loss Gets Harder During Menopause

Why Weight Loss Gets Harder During Menopause
Three years ago, dropping 10 pounds before a wedding took six weeks. You ate less, moved more, and boom, results. Last summer, you tried the same approach and barely moved the scale at all. The diet was the same. The exercise was the same. Your willpower was, if anything, better. What’s going on? You’re not imagining it, you’re not failing, and your body isn’t broken. Menopause just changed the rules, and no one warned you. This article explains what actually changed, why, and what it means for your results.
Here’s the short version: fat loss gets harder during menopause because of what we call the GFIT 5 Shifts of Menopause: estrogen decline, accelerated muscle loss, rising insulin resistance, disrupted sleep, and elevated baseline cortisol. Each one alone would make things harder, but all five, compounding is what makes the old playbook useless. Understanding the biology at play is the first step. The plan that actually works after menopause is built around this biology, not against it.
Want a plan built for your stage of menopause?
Book a free 15-minute consult with our Winnipeg menopause coaching team. We'll map your specific shift profile, explain what's driving the stall, and confirm your insurance coverage on the call.

The GFIT 5 Shifts of Menopause
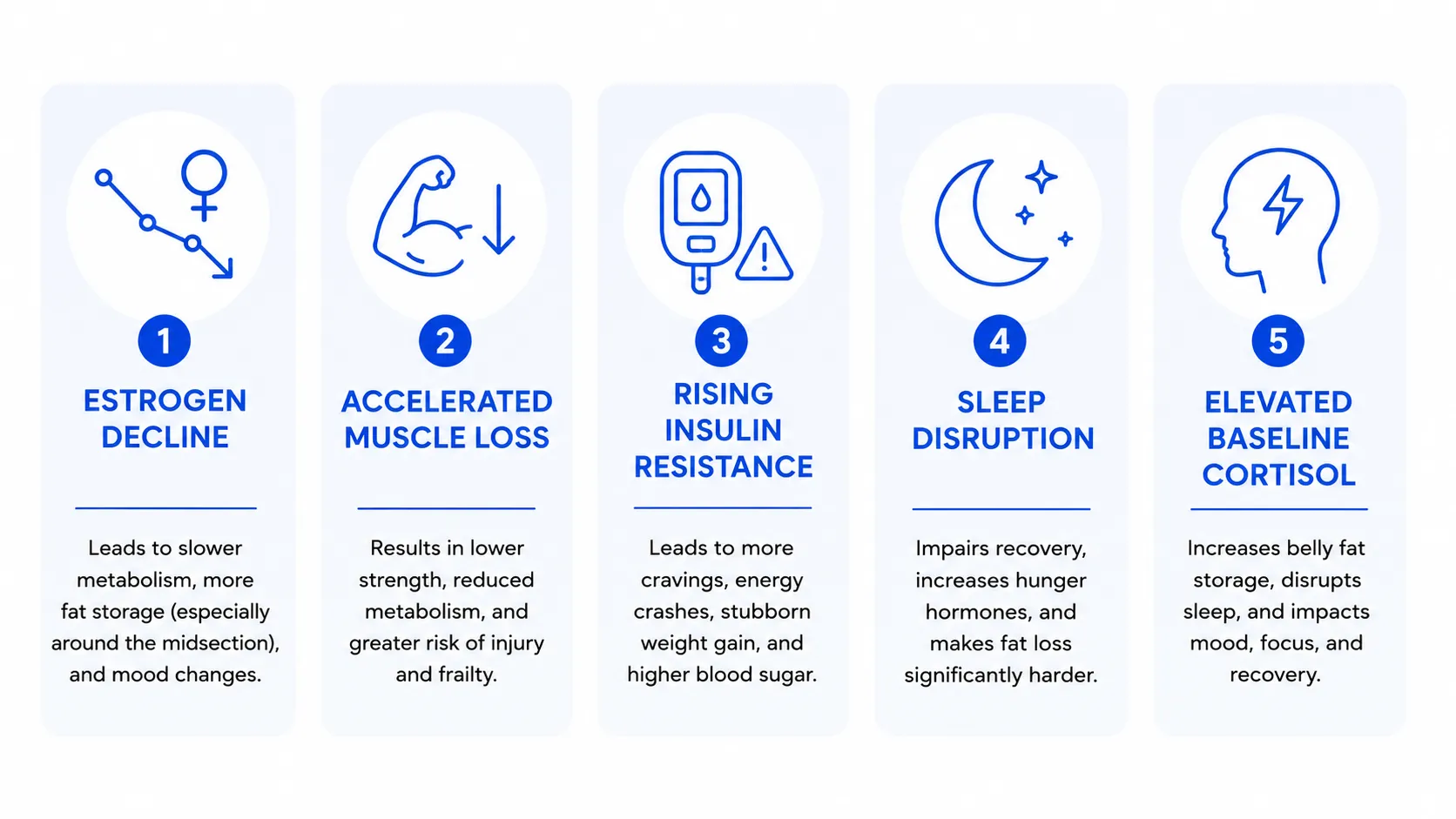
1. Estrogen decline
Estrogen is not just a reproductive hormone: it plays an active role in insulin sensitivity, fat distribution, muscle protein synthesis, satiety signalling, and bone density. When estrogen levels drop during perimenopause, and again at menopause, the body responds across every one of those systems.
Three downstream effects matter most for weight:
- Fat redistribution. Estrogen historically directed fat storage toward the hips and thighs. But as it declines, fat stores tend to shift more towards the abdomen, where it is more metabolically active and more strongly linked to insulin resistance and cardiovascular risk.
- Muscle protein synthesis declines. The same protein-heavy meal builds less muscle after 40 than it did at 35. This compounds with the muscle loss point below.
- Satiety signalling weakens. Many women in menopause report being hungrier sooner after meals, and less satisfied by the same volume of food.
2. Accelerated muscle loss
Sarcopenia (age-related muscle loss) starts in your mid-30s and works against you to start decreasing muscle mass at about 1% per year. In perimenopause and menopause, the rate accelerates. By age 60, a woman who has not actively strength trained may have lost 20 to 30% of her peak muscle mass.
Muscle is metabolically active tissue. It burns calories at rest, sinks blood glucose, improves insulin sensitivity, and supports the joint stability that lets you stay active. Lose enough of it, and your resting metabolic rate drops by 100 to 200 calories per day. That alone is enough to convert what used to be a deficit into maintenance, or maintenance into slow gain.
3. Rising insulin resistance
Estrogen helps muscle cells respond to insulin. As estrogen declines, insulin sensitivity declines with it. The same carbohydrate-rich meal that produced a normal blood sugar response at 40 may produce a higher, longer-lasting spike at 52. Higher insulin signals fat storage and suppresses fat release.
This is why many women in menopause start noticing that carbs they used to tolerate now make them feel different. Energy crashes after meals, midsection bloat, and a noticeable preference for storing weight around the belly are all signals of this hormone shift.
4. Sleep disruption
Vasomotor symptoms (hot flashes and night sweats), declining progesterone, and the 3 am wakeup pattern most perimenopausal women describe all conspire to fragment sleep. The cost is not just feeling tired, it directly affects your body composition.
Fragmented sleep raises ghrelin (the hunger hormone), lowers leptin (the satiety hormone), elevates cortisol, impairs glucose tolerance, and reduces motivation to exercise. A single night of poor sleep can reduce your next-day calorie burn by 5 to 20%, and increase appetite by 200 to 400 calories. Multiply that across years of disrupted sleep, and the cumulative effect on weight is enormous.
5. Elevated baseline cortisol
Cortisol is not the villain it is often made out to be. The problem is not the cortisol itself. It’s the chronic elevation that never returns to baseline. In menopause, declining estrogen, fragmented sleep, and a tendency toward slower stress recovery all push your baseline cortisol up. And chronically elevated cortisol drives midsection fat storage, breaks down muscle, disrupts sleep further (creating a feedback loop), and increases cravings for high-calorie, high-carb foods. The afternoon energy crash, followed by intense carb cravings that many menopausal women describe, is a cortisol pattern, not a willpower failure.
"The women I work with come in convinced something is wrong with them. But honestly, they’re just running a 2025 body on a 2010 operating system. Once we update the operating system, the body responds in an amazing way, usually within the first six weeks." April Klippenstein, GFIT menopause coach
The Compounding Effect (Why Each Shift Alone Is Manageable, But All Five Together Is Overwhelming)
Any one of these shifts would be manageable. Estrogen drops? Add a little more protein and strength training. Sleep gets disrupted? Tighten the wind-down routine. Cortisol creeps up? Walk more and lift slightly heavier.
The challenge in menopause is that all five shifts happen at once, often within the same 6 to 18-month window. The body that worked fine on autopilot for two decades suddenly demands a completely different input profile, all at the same time. And because nobody told you the rules changed, you keep doing what used to work, but getting less and less back from it. It’s incredibly frustrating.
But honestly? The women who thrive during menopause are almost never doing just one big thing. They are doing five medium things consistently. Strength training, plus protein, plus sleep, plus less alcohol, plus daily walking. None of them are dramatic shifts, but all of them done consistently have dramatic results.
Perimenopause vs Menopause: Where the Difference Matters
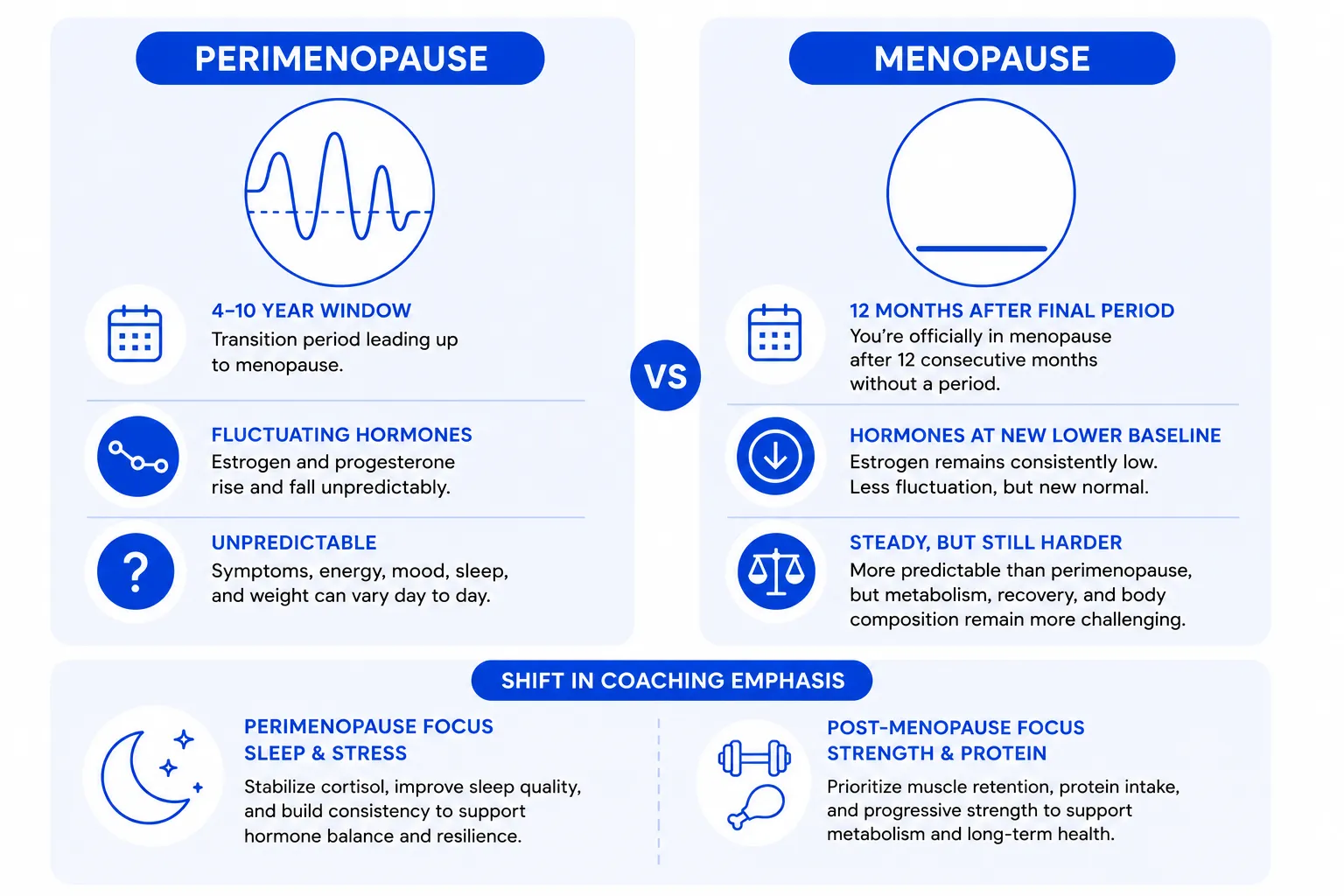
Perimenopause is the 4 to 10-year window leading up to menopause, typically starting in the early to mid 40s. Hormones fluctuate dramatically during this window, which is why symptoms (and weight) can feel unpredictable. One month you’re totally fine, and the next month you can’t sleep, have hot flashes, and the scale jumps three pounds for no reason.
Menopause is the date 12 months after your final period. After menopause, hormones stabilize at a new, lower baseline. The wild fluctuations stop, but the lower estrogen, lower progesterone state is now permanent. Weight management challenges shift from unpredictable to steady (but still harder than before).
The plan that works is similar across both stages, but the emphasis shifts. In perimenopause, sleep and stress are the biggest levers because hormone fluctuation amplifies their effect. Post-menopause, strength training and protein become even more important because without the cyclic estrogen exposure, muscle loss accelerates.
What This Means for Your Weight Loss Plan
Three principles that apply regardless of which stage you’re in:
- Protein at every meal, hitting 1.4 to 2.0 grams per kilogram of bodyweight per day.
- Strength training twice per week minimum (three is better, but more than that often isn’t).
- Sleep and stress are treated as non-negotiables, not nice-to-haves.
For the full action plan, including the specific moves and the four things that stop working after 40, see our sibling article that is built around exactly this.
When to Consider HRT (And When to Consider a Coach)
Hormone Replacement Therapy is not a weight loss intervention, but for many women, it makes weight loss meaningfully easier by stabilizing sleep, mood, vasomotor symptoms, and energy. The decision to start HRT is a conversation with your physician based on your full symptom picture, your medical history, and your risk profile.
Coaching enters the picture when the changes you need to make are clear in theory, but hard to execute alone. Three signs you should bring in help:
- You’ve read articles like this one and tried the changes, but life keeps disrupting consistency.
- You’re navigating the symptoms of perimenopause (sleep, mood, hot flashes) alongside the weight question, and they feel hard to decode alone
- You want a Winnipeg-based program that coordinates with your physician on HRT and your fitness program in one place.
Our menopause weight loss coaching at GFIT is built specifically for this transition. Most Winnipeg clients are insurance-covered through Manitoba Blue Cross, Canada Life, Sun Life, Manulife, or Green Shield, which means a typical 12-week program runs little to nothing out of pocket if you have benefits.
One of our Winnipeg clients, Margaret, came to us at 53, two years post-menopause and 18 pounds heavier than she had been at 48. Her doctor had ruled out thyroid and other medical causes, yet she was really struggling with body image and poor self esteem. To her surprise, we didn’t put her on a diet. We added two strength sessions per week, raised her protein to 140 grams per day, tightened her sleep routine, and reduced alcohol to one glass per week. Six months later she had lost 14 of the 18 pounds, and she described herself as "stronger than I have been in 15 years."
Tired of running a 2025 body on a 2010 operating system?
Book a free 15-minute consult with our Winnipeg menopause coaching team. We'll map your specific shifts, build a 90-day plan around them, and confirm your insurance coverage on the call.
Frequently Asked Questions
No! The biological shifts make weight gain more likely if you continue doing what worked in your 30s, but the shifts are entirely manageable with the right inputs. Women who strength train, eat enough protein, sleep well, and limit alcohol typically maintain their weight through menopause and (more importantly) often improve their body composition.
Population averages typically show 5 to 15 pounds of fat gain during the menopause transition, with most of the gain settling around the midsection. But remember this is an average, not your destiny. Women who change their approach to match their biology often maintain their weight or lose weight during this window; women who keep doing what used to work typically land in the upper range of average gain.
HRT is not a weight loss drug, and most studies show it produces modest direct effects on weight. The bigger effect is indirect: HRT often improves sleep, mood, hot flashes, and energy, all of which make it dramatically easier to follow a sustainable weight loss plan. The decision to start HRT is between you and your physician based on your full symptom picture, not just weight.
Estrogen historically directed fat storage toward the hips and thighs. As estrogen declines in menopause, that signal weakens and fat is preferentially stored in the abdomen. The abdominal fat is more metabolically active and more linked to insulin resistance, which creates a negative feedback loop. Strength training, adequate protein, sleep, and reducing alcohol are the most effective levers to reverse this pattern.
Yes! And many of our clients do. Post-menopause weight loss is slower than what you remember from your 30s, but it is fully achievable with the right approach. Realistic targets are 0.5 to 1 pound per week of fat loss while preserving or building muscle. The body composition change at the same scale weight is often more visible than the scale change.




Book a call with our Wellness Coordinator to learn more



